
EXPAREL Provides Pain Relief When It Matters Most
EXPAREL in Pediatric Surgery
Approved for Postsurgical Pain Management in Pediatrics
The first and only FDA-approved long-lasting local analgesic for ages 6 and above.1 Demonstrated in PLAY, a clinical trial centered uniquely on safety in children.2 Pediatric patients in the EXPAREL study were defined as 6 to less than 17 years of age.
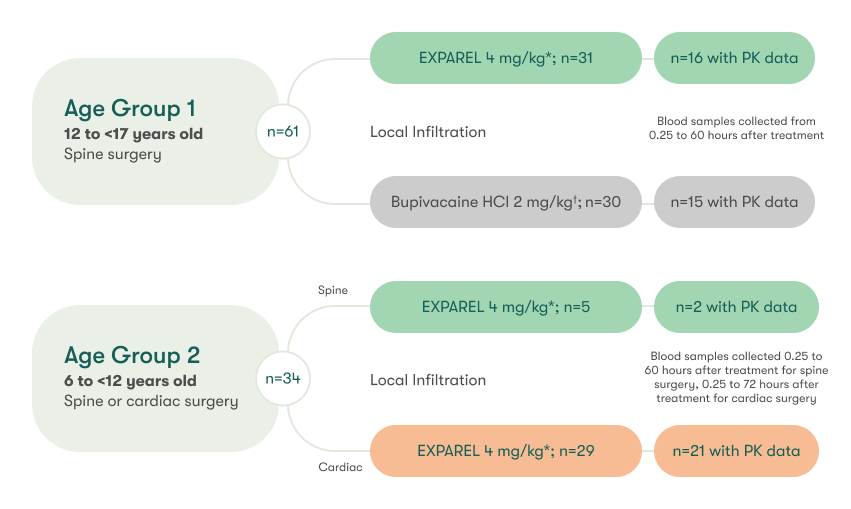
The PLAY Study Was Designed to Establish the Safety & Pharmacokinetics (PK) of EXPAREL in Pediatric Patients3
A multicenter, open-label, phase 3 trial with 2 parts including pediatric patients 6 to <17 years of age
Swipe left on table to see more
Study End Points
Part 1: PK and safety
Part 2: Long-term safety
- AEs up to 30 days after surgery
- Neurologic assessments
- Clinical laboratory tests
- Vital signs
Baseline characteristics were generally comparable among groups
*Maximum total dose of 266 mg
†Maximum total dose of 175 mg
The Safety of EXPAREL Was Comparable to Bupivacaine & Consistent Across Treatment Groups
EXPAREL was well tolerated for all age groups, with TEAEs being mild or moderate and no discontinuations3
Overview of TEAEs With EXPAREL Greater Than or Equal to 10%
| Patients aged 6 to <17 years old | Patients aged 6 to <12 years old | |
|---|---|---|
| Spine surgery EXPAREL 4 mg/kg; n=36 (%) | Cardiac surgery EXPAREL 4 mg/kg; n=29 (%) | |
| Vision blurred | 7 (19.4) | 1 (3.4) |
| Constipation | 9 (25) | 4 (13.8) |
| Nausea | 11 (30.6) | 2 (6.9) |
| Hypoesthesia oral | 4 (11.1) | 0 |
| Vomiting | 10 (27.8) | 4 (13.8) |
| Anemia postoperative | 5 (13.9) | 0 |
| Muscle spasms | 4 (11.1) | 0 |
| Hypotension | 4 (11.1) | 0 |

Swipe left on table to see more
There were no treatment-related cardiac or nervous system adverse events in the EXPAREL arms4
There is not enough evidence to determine if the numbers associated with spine surgery in patients aged 12 to <17 years old are indicative of differences in the surgery types
TEAE, treatment-emergent adverse event.
For Children, a Non-Opioid Option Should Be the Only Option
The risks and complications of adult-based pain management approaches may be magnified in children.5 Opioids, short-acting local anesthetics, and delivery devices are the mainstay despite safety implications and limited studies in children.5
Even So...
50% of Children
report moderate to severe pain in the hospital after surgery6
~20% of Children
report chronic pain 12 months
after surgery6
Opioids can be attributed to 50% of postsurgical respiratory failure events in children and may also hinder recovery, extend hospital stay, and negatively impact both patient and parent experience.7-9
Potential Side Effects & Complications With Current Modalities
Opioids5
- Nausea/vomiting
- Constipation
- Urinary retention
- Cognitive impairment
- Dependence
Device-Based Platforms (ie, Pumps and Catheters)
- Accidental removal10
- Overdose11
- Leakage12
- Infection10
- Unpredictability or malfunction10-12
Societies Recommend Opioid-Minimizing Pain Management Platforms
Medical societies recommend non-opioid analgesics and a multimodal approach to pain management for pediatric patients13
American Society of Anesthesiologists
Task force on acute pain management14
Analgesic therapy [for pediatric patients] should depend upon age, weight, and comorbidity, and unless contraindicated should involve a multimodal approach.


Society for Pediatric Anesthesia
Guidelines from the Society of Pediatric Anesthesia15
…clinicians should use all methods possible to minimize the use of opioids… Use of nonopioid analgesia is encouraged including regional analgesia techniques…
JAMA
Expert panel* guidelines that include the American College of Surgeons Education Committee16
…healthcare professionals caring for children who require surgery must recognize the risks of opioid misuse associated with prescription opioids, [and] nonopioid analgesic use should be optimized in the perioperative period…
*This guideline was developed by the American Pediatric Surgical Association Outcomes and Evidence-Based Practice Committee, in addition to a geographically diverse multidisciplinary team composed of leaders in pediatric opioid stewardship from academic and community hospitals and representatives from the American College of Surgeons (ACS) Education Committee, the American Academy of Pediatrics Section on Surgery, pediatric anesthesia, pediatric nursing, general surgery residency, pediatric surgery physician assistants, and addiction science.17
AE, adverse event; FDA, US Food and Drug Administration; JAMA; Journal of the American Medical Association.

